The remainder of this article will seek to scientifically answer the following questions based upon the best data available: How fast will the will the Ebola virus spread? How long will it take for Ebola to reach its apex? Will the transmission rates for Ebola be the same in the United States as it is/was in West Africa? Finally, what are odds of contracting virus?
Relative Mortality Rates Compared to Contracting Ebola

Data sources: David Ropeik/Harvard University, National Weather Service, World Health Organization, Northeastern University Laboratory for the Modeling of Biological and Socio-Technical Systems, National Geographic, United States Census
Although the odds of one in five thousand does not sound like dangerous odds for contracting Ebola by traveling to Monrovia, but traveling to Monrovia is much more fatal than being struck by lightening and dying in a car accident. Please pause and savor the moment. This graphic, listed above, is the best news that I have to offer about the transmission rates of Ebola.
When we compare the Ebola transmission rates of Ebola to other pathogens, the number two, which represents the number that one Ebola patient will expose and infect two others with the virus. In other words, according to the CDC and if we use statistical modeling, one Ebola patient will infect and average of two people, which in turn infects two more each and so forth.
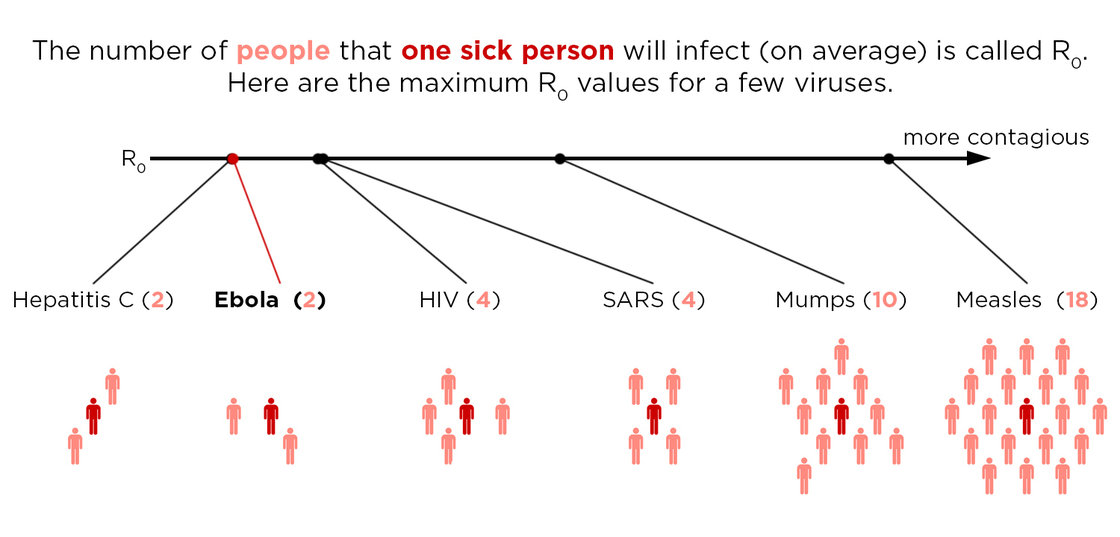
This chart, derived from CDC numbers, is supposed to make the public feel better. It would seem that the chart shows that Ebola really poses only a small danger because its reproductive rate (Ro) is less than other pathogens. This is almost an irrelevant point. Unless a burnout of the virus is achieved, any virus will reach a point of exponential Ro growth in which two patients infect four, who in turn infect 16, etc. So what is the burn out rate for Ebola? The simple answer is very disturbing, nobody knows. In an article published on the Washington Post website, the CDC gave the Post exclusive access to its statistical models and projections. The only valid statement that could be made by the Post is that transmission of the virus will continue until the Ro rate slips below one transmission for every infected person. Since we are still within the first generational cycle of Ebola transmission within the United States, this is not a reassuring position being offered by the CDC.
The CDC’s “Power of Two” Defines the Transmission Rate of Ebola
Let’s take the CDC at their word and project the Ro rate for Ebola to be two. As an aside, later in the article, a case will be made which demonstrates that this number is far too low when it comes to the United States.
If we can envision a scenario in which two patients infect four and four patients infect 16, this is how Ebola’s R0 rate would progress.
First generation of exposure of one Ebola patient = 2 new Ebola patients
Second generation of exposure of two Ebola patients = 4 new Ebola patients
Third generation of exposure of four new Ebola patients = 16 new Ebola patients
Fourth generation of exposure of 16 new Ebola patients = 256 new Ebola patients
Fifth generation of exposure to 256 new Ebola patients = 65,536 new Ebola patients
Second generation of exposure of two Ebola patients = 4 new Ebola patients
Third generation of exposure of four new Ebola patients = 16 new Ebola patients
Fourth generation of exposure of 16 new Ebola patients = 256 new Ebola patients
Fifth generation of exposure to 256 new Ebola patients = 65,536 new Ebola patients
Sixth generation of exposure to 65,536 patients = 4,294,967,296 new Ebola patients
What Is the Life Cycle of Ebola?
As a point of definition, one must ask the question: How long is an Ebola life-cycle? If one knows the Ro rate coupled with the life cycle of the illness, we can calculate its spread. The virus incubates from 2 to 21 days according to the CDC. The virus claims its victim in a range from 6 to 16 days. Taking the median measure of both variables, we can calculate that the average Ebola life cycle is 20 days.The long side of the Ebola life cycle is 37 days. This could be viewed as the maximum time between the onset of exposure and the time of death.
The short side of the Ebola life cycle is 8 days.
I have decided to error on the side of being conservative and will use the combination of median times associated with exposure to expiration of the patient which is 20 days. However, the high end estimate for the life of an Ebola life cycle is 37 days. Therefore, for our purposes of analysis,the Ebola life cycle will be fixed at 30 days, which is a very conservative estimate. Further, the following estimate is based upon the unproven belief that Ebola cannot be transmitted until the carrier is symptomatic. For now, we will ignore the fact that Ebola is almost assuredly transmissible during the incubation period.
The next step in answering the question is how fast will Ebola spread through, not just the United States, but also through the world? I have scoured various data bases and have concluded that this information is not readily available. I have a hard time believing that the CDC and the CIA have not run their own set of projections. Unfortunately, the public will never have access to this information. Yet, I do think there is enough data to make some crude estimates.
If we take the CDC figures at their word in that every Ebola patient infects two people, and we know the mortality rate for contraction of the virus is about 70%, then we can make some raw number projections. Using the power and projections of two and subtracting the survival rate for Ebola, we can project that about 2.85 billion are going to die world-wide within six Ebola generations, or roughly in about six months. Since the U.S. makes up a little less than 5% of the global population, this means that we could expect to see 140 million Americans dying from the Ebola virus.
SUBSEQUENTLY, YOUR ODDS OF CONTRACTING EBOLA BASED UPON THESE PROJECTIONS IS 44% WITH A SURVIVAL RATE OF 30%
Thomas Duncan died on October 8, 2014. This would place the United States’ first Ebola generational cycle back to September. By January, the announced month that the CDC says that the GSK vaccine will be ready, the country will be one month away from the apex of the spreading of Ebola. Does anyone else believe in coincidences? One would have to be a coincidence theorist to not believe that this event is being orchestrated. If you think this viewpoint to be extreme, did you know that after the Spanish Flu Pandemic in 1918, that companies like Lysol and Vicks Vapor Rub made money hand over fist? From previous articles, I have established that the CDC owns the patent on Ebola and the NIH owns the patent on the Crucell vaccination that was tested on human subjects in 2006. It has always been the case that one man’s misfortune is another man’s payday.Is September the correct month establish ground zero when it comes to calculation the R0 rate? Maybe. I am not sure the United States has experienced the first generational effect of Ebola in which we have seen two patients die from Ebola after having infected four other people. There are allegations of CDC coverup as well as the disappearing of people who potentially have the virus. Therefore, we cannot be sure that we have positively entered the danger zone. Yet, it is safe to say that by the time we get to next summer, I believe the apex of the Ro for Ebola will have been reached.
GDP As a Predictor of Ebola’s Ro
Ask yourself these common sense questions regarding the Ro rate of Ebola: In which type of economy will Ebola likely spread the fastest? Will Ebola spread the fastest in an agricultural environment, or in industrial based economy? What increased dangers of being primarily a service economy pose to the Ro rate in places like the United States?
As a result of these questions, I formulated a hypothesis which postulated that the economic base and GDP of a nation could be correlated with the Ro rate of Ebola. I have done the research and in all statistical honest, the question is still somewhat open because the number of nations and their respective economies is still small. However, the trend curve is undeniable. What jumps out as a result of this investigation is that a rural based, low GDP economy has a much a slower rate of transmission that does an industrial economy. This leads rise to the distinct probability that nations with large service economies will spread the virus faster and the expected Ro rate will be far higher than the CDC, one-size-fits-all figure of the Ro rate of tw0. Why?
This is a simple matter of math. In a rural agricultural economy the number of people that a potential Ebola carrier will come into direct contact with is small. There are not many group gatherings, no concerts, dining out is not common, going to movie theaters and large sporting events is uncommon in these cultures. However, industrialization begets urban development. And with that comes public transportation on a daily basis. Urban dwellers come into far more contact with people because they attend movies, concerts, go to shopping malls and sporting events. The number of people that city residents come into contact with on a daily basis is far higher than for rural residents. In a service economy, such as the U.S., the Ro should be more dramatic. Does the data support the conclusion? In a word, yes.
I am surprised that Dr.Althaus did not make the following connection. The Ro rate for Ebola is correlated with GDP. The differential rates between Sierra Leone and Liberia are not insignificant. Sierra Leone has an Ebola Ro which is 60% higher than Liberia. The economic difference speaks to why Sierra Leone has a higher Ro.
GDP (purchasing power parity) LIBERIA
$2.898 billion (2013 est.)
$2.681 billion (2012 est.)
$2.475 billion (2011 est.)
note: data are in 2013 US dollars
SIERRA LEONE
$9.156 billion (2013 est.)
$$8.079 billion (2012 est.)
$7.016 billion (2011 est.)
note: data are in 2013 US dollars
GDP – composition by sector agriculture: 76.9%
industry: 5.4%
services: 17.7% (2002 est.) agriculture: 47.9%
industry: 18.6%
services: 33.5% (2013 est.)
Liberians will come into contact with fewer people because of the more primitive nature of their economy. As a factor of GDP, Sierra Leone will have more restaurants, shopping malls, etc. It makes sense that Sierra Leone will have higher transmission rates.
The Sierra Leone economy is estimated to be at .05% of the United States. What does this say about the R0 rate of the United States? Until the nation is shut down because of the virus, the U.S. transmission rates will far higher than it is in Africa. The rate certainly will not be two. In this scenario, the country and its economy will be shut down in months.
Conclusion
The data speaks for itself. The fact that the President and the CDC did not shut down air travel from West Africa and the fact that the border is still wide open, is inexcusable and can legitimately be used to call into question the motives of the CDC, the NIH and the President.
There has been much made in the alternative media that the Ebola virus is a hoax. The only way, at the moment, that this claim can be substantiated is to get one’s hands on lab samples and perform an analysis. Until this can be done, that claim is pure conjecture. However, if Ebola fails to spread in the manner described above, then we can conclude that this is not Ebola, but rather, a bioweapon. And of course, if a legitimate vaccine could be developed and widely distributed, the spread could be slowed. However, how can we trust a vaccine that is so hastily put together? In five, ten and even twenty years, what would be cancer rate for such a vaccine which could be experienced as a side effect?
By not shutting down the airports to West African travel, the President is playing Russian Roulette with our collective futures. If the virus does spread as expected, then this would explain the HHS documents describing camps to house Ebola victims in. It also would explain all the FEMA disaster drills. We could be months away from the point of no return. Are you ready for what is coming. Can you self-quarantine and have enough supplies, along with a way to protect these supplies, long enough to survive?
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.